
Is Esomeprazole the solution to your heartburn? Find out here
If you're reading this, maybe your stomach needs some relief. Have you felt any burning? Heartburn or pain near your breastbone? If the answer is yes, you probably have a gastric ulcer and don't know it.
Gastric ulcers are deep wounds of the mucous membrane that covers the walls of the stomach. They are the result of many things, and their most common symptom is a non-specific, dull pain in the mouth of the stomach.
Between 5 and 15% of people suffer from a gastric ulcer, but as specialists, we know that this number is higher. The incidence of gastric ulcers depends on the extent of the diagnosis.
The diagnosis of gastric ulcers is tricky since not all people show symptoms according to specialists around the world; therefore, not all people go to the doctor to have an endoscopy.
The gastric ulcer also called peptic ulcer or gastroduodenal ulcer (when it also involves the duodenum), takes its name according to the place where it appears, being the duodenal ulcers the most frequent, especially in the west of the world.

Did you know that the intake of NSAIDs is a risk factor for the development of peptic ulcers? Yes, taking analgesic or anti-inflammatory drugs such as acetaminophen or ibuprofen increases the risk of developing a gastric ulcer and is today the principal cause.
Excessive and uncontrolled consumption of NSAIDs (non-steroidal anti-inflammatory drugs) triggers a series of chemical activities that eventually end up damaging the epithelium covering the stomach. When we take an acetaminophen or ibuprofen pill, there is an inhibition of natural agents that protect our stomach, allowing gastric acid to damage the cells in the walls.
There are also other common causes, such as infection by the bacterium Helicobacter pylori, which lives naturally in our digestive system, but leads to symptoms and damages our stomach when it gets out of control.
Other evidence shows that there may be genetic factors related to peptic ulcer disease. Research linked to family groups showed that these ulcers are two or three times more frequent in first-degree relatives than in the rest of the population. Interesting, isn't it? So be careful with your loved ones if you suffer from gastric ulcers.
The treatment of a gastric ulcer consists of allowing the damaged area to heal, avoiding complications. When it comes to medical treatment, the options are many depending on the cause, but there is one medication in common that can never be missing from any treatment scheme; the proton pump inhibitor.
Proton pump inhibitors (PPIs) are the treatment of the first choice in peptic ulcer disease because they are the most potent antisecretory drugs on the market.
Antibiotic medications may be added, depending on whether the cause of the ulcer is an infection or not.
We speak about the commonly called ''gastric protectors'' when we say proton pump inhibitors, such as Omeprazole, Esomeprazole, Lansoprazole, Pantoprazole and Rabeprazole. We will now explain more about Esomeprazole, the strongest and effective pump inhibitor.
What is Esomeprazole?
Nexium® is a proton pump inhibitor derived from omeprazole that is responsible for reducing the amount of acid secretion in the stomach. Its primary function is to protect the stomach lining from gastric acid since the latter interferes with the healing process of the gastric ulcer.
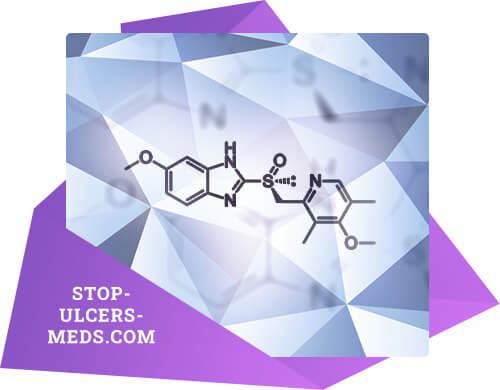
Esomeprazole is the first pump inhibitor produced in the form of isomers in order to provide significant therapeutic benefits compared to conventional omeprazole.
Isomers are elements that have the same molecular formula but differ in the nature or sequence of binding of the atoms that make up the isomer.
This drug was formulated so that both its metabolism and absorption were more uniform and durable than Omeprazole; consequently, its pharmacological action is more effective and longer-lasting.
How does Esomeprazole work?
To make things simple, we must first know a few things: the normal function of the stomach and what happens during a gastric ulcer.
To begin with, we must know the natural composition of the stomach, which is made up of different layers: mucosa, submucosa, muscular layer, and serosa. Each one of them has a specific and vital function in our digestive tract.
Today we will talk mainly about the mucosal layer. The mucosal layer is composed of various cell groups, the epithelial cells being the most important for this discussion.
The epithelial cells are found in the stomach in greater quantity, and their purpose is to protect the mucosa thanks to the release of a viscous substance called mucus together with bicarbonate.
The epithelial cells are found in higher amounts in the stomach, and their purpose is to protect the mucosa thanks to the release of a viscous substance called mucus together with bicarbonate. These last two elements are incredibly valuable because they antagonize gastric secretions and protect the rest of the layers of the stomach.
Another essential cell group is the parietal cells, which make the perfect match to the epithelial cells. These cells have the role of producing and releasing hydrochloric acid in the stomach, the main tool for the absorption of the food we consume daily.
The parietal cells (also called oxyntic cells) are responsible for sustaining an acidic pH in the stomach so that it is always ready for digestion. This release of gastric acid happens through peaks during the day, so when we wake up, we are hungry because our stomach produces more hydrochloric acid, and after eating, we feel relief from those silly cramps.
Now, why do we want to know this? Well, we are interested in learning this because the ulcerative problem takes place when the mucosal layer is injured, losing its ability to protect the rest of the layers.
The acid produced by the parietal cells can corrode the deeper walls when the protective mucosa is worn away; leaving a deep, rounded wound known as the gastric ulcer.
Esomeprazole acts by inhibiting the secretion of hydrochloric acid from the parietal cells, to allow the damaged area to recover through the spontaneous healing of its cells.
When Esomeprazole enters the body, it is responsible for blocking specific receptors on the surface of the parietal cell membrane. This drug stops the proton pump ATPase-H/Na.
The ATPase pump is, as its name suggests, a small receptor placed on the membranes of the parietal cells that is responsible for pumping the hydrogen ions to the gastric surface to maintain the natural acidic environment.
Indications and contraindications When should I take Nexium®?
We must be honest before starting this section and tell you the truth: only medical professionals can prescribe this medication.
Do not take Esomeprazole if you do not need it. Do not take Esomeprazole if a friend, co-worker, or family member has recommended it to you. This medication has specific indications, so it should not be taken lightly.
It should be started according to medical criteria under the following conditions:
- Peptic ulcer: H. pylori or NSAIDs.
- Gastroesophageal Reflux Disease.
- Functional Dyspepsia.
- Zollinger-Ellison syndrome by tumors.
- Prevention of peptic ulcers by treatment with NSAIDs or by stress.
Gastroesophageal Reflux Disease (GERD) is another common indication for Esomeprazole. It is a condition similar to ulcers caused by an increase in the gastric acid, but in this particular case, the acid affects both the stomach and the esophagus.
This disorder is caused by the leakage of gastric contents into the esophagus, damaging its muscular walls and causing inflammation of the esophagus (esophagitis) from reflux.
Functional dyspepsia is a term used to include all the signs and symptoms of indigestion that occur frequently and without apparent cause.
Zollinger-Ellison syndrome is a very unusual condition caused by the growth of one or more tumors in the pancreas or duodenum that consequently release excessive amounts of gastrin, promoting acid secretion from the stomach.
Gastrin is a hormone released in the body to stimulate or regulate the production of hydrochloric acid. There is an overstimulation of the parietal cells when it is released in excess, producing an overly acidic gastric environment.
Contraindications:
Like any other medication this is not indicated for persons with increased sensitivity to the active component, in this case, Esomeprazole, benzimidazole, or any of the ingredients of the pharmaceutical formulation.
There are situations where it can be taken with caution and under strict medical supervision:
Pregnancy:
Despite fervent research, clinical data on the risks of Esomeprazole in pregnancy are insufficient. However, its use is advisable only when necessary and under medical supervision.
Breastfeeding:
This drug does pass into human breast milk, finally confirmed during 2020; however, it does so in quantities not significant enough to cause an effect on the baby.
It has not been proven yet to date that children have any problems from consuming milk with Esomeprazole components. It is also not suggested to use Esomeprazole during breastfeeding. This can only be prescribed by a doctor and only when needed, even if the effects are not significant.
In elderly:
Esomeprazole increases the risk of spontaneous hip, wrist, and spinal fractures, mainly when used for a long time (one year or more).
We all want to reach healthy, fit, and lucid elders; however, predicting this is often impossible. Taking care of your health is your task, your commitment to yourself. One thing we can control is the health of those who are already going through senescence.
The elderly are people who enjoy a not so optimal organism, and one of the organs that suffer most during this stage is the bones. During the old age, a wearing down of the bones occurs, considered normal due to aging.
The consumption of Esomeprazole in the elderly should be allowed only when needed and not for long, since as we know, it increases the impairment of the bones of those we most want to be healthy. We must be aware if we wish to take care of their health!
Side effects: The safer, the most effective!
This drug is generally well tolerated and considered quite safe; however, there are some situations where certain people have been affected by this medication. All proton pump inhibitors are highly effective in treating the above conditions; however, they are not risk-free, like any other drug.
Side effects can be grouped into very common, common, rare, and very rare. We can draw up a table by organs and systems from this information to make it easier for you:
| Affected system | Estimated frequency | Side effects symptoms |
|---|---|---|
| Gastrointestinal | Frecuent | Abdominal pain, diarrhea, nausea |
| Nervous system | Frecuent | Headache |
| Metabolism and nutrition | Less frequent | Swelling |
| Liver and bile ducts | Less frequent | High liver enzymes |
| Skin and subcutaneous tissue | Rare. Very rare | Hair loss, high sensitivity to light, skin inflammation, itching, hives. |
| Blood and lymph nodes | Very rare | Disorders in blood cells: leukopenia, thrombocytopenia, pancytopenia or agranulocytosis |
Rare mental disorders such as difficulty sleeping, agitation, confusion, depression or hallucinations are also known.
Among other rare symptoms we can mention taste alteration, blurred vision, vertigo, breathing problems, dry mouth, hepatitis or liver failure, muscle weakness and joint pain.
Also described are extremely rare disorders such as impaired kidney function, excessive sweating, muscle aches, and decreased blood salt (hyponatremia).
Another important consideration is that this drug increases the blood levels of gastrin, and therefore it can cause hypergastrinemia; however, this fact lacks scientific soundness, and more studies are needed to confirm these data.
As we have already mentioned, this drug tends to be very well-tolerated, and its side effects are rare, usually appearing after six months of continuous treatment at the most.
Interactions with other drugs:
Have you ever wondered how the drug gets to the precise site of the disease? The medications do not travel to the exact place where the injury is but instead spread throughout our bodies, resulting in interactions and side effects in other organs.
An interaction is considered to exist when the effects of a drug are modified by the simultaneous presence of another drug, a plant preparation, food, drink, or some environmental chemical.
Esomeprazole is metabolized in the liver once consumed, and its specific enzymatic pathway is that of the CYP2C19 complex so it can interact with the metabolism of other drugs using this same system.
Drugs that use this same hepatic pathway for their metabolism are diazepam, citalopram, imipramine, clomipramine, phenytoin, clopidogrel, and voriconazole, so simultaneous use with Esomeprazole is not advisable.
Esomeprazole interacts with some drugs that suppress protease enzymes (mainly antivirals) such as amprenavir, atazanavir, indinavir, lopinavir, ritonavir, etc. In this case, the concomitant use of esomeprazole causes a substantial decrease in the antiviral in the body, making it less effective.
Methotrexate is a drug used for serious diseases and even cancer. An increase in methotrexate can occur when used in combination with Esomeprazole; however, this is not a widespread fact that commonly happens when the former is used in high doses.
Esomeprazole also interacts with tacrolimus. Tacrolimus is an immunosuppressive drug used in patients with excessive immune system activity. When tacrolimus and esomeprazole are taken together, an increase in blood amounts of tacrolimus occurs, enhancing its side effects.
As Esomeprazole is a drug that influences gastric acidity, it can also indirectly change the absorption of other pH-dependent medications in the stomach. These pH-dependent drugs are ketoconazole, itraconazole, erlotinib, and iron salts.
Although the relationship between amoxicillin, quinidine, and esomeprazole has been extensively studied, it has not been confirmed to date. Esomeprazole does not represent a risk in the absorption of these drugs; on the other hand, it can work as a gastric protector in the long treatments of these drugs.
The same happens with drugs such as Naproxen or rofecoxib; scientific results are not relevant enough to establish a close relationship that could determine the interaction between the two drugs.
How should I take Nexium®?
You must take into account that the dosage plan explained below may change depending on the needs of each person and the opinion of each doctor.
We recommend that you first consult with your doctor about the administration and dosage schemes before starting this medication.
As mentioned in the first sections, management may change depending on the cause of the ulcer or the disease. Treatment includes taking antibiotics with pump inhibitors if the ulcer is due to H. pylori bacteria, but if not, pump inhibitors only are enough.
Dosage in Gastroesophageal Reflux Disease (GERD)
The main plan is 40 mg per day for four weeks. You should continue for four more weeks in case the symptoms have not improved after the first four weeks.
20 mg per day is suggested to avoid recurrences in long-term control of esophagitis.
Dosage in H. pylori infection
Either to promote healing of an ulcer induced by the bacteria or to prevent the reappearance of ulcers in patients with a history of H. pylori the suggested plan is 20 mg every twelve hours (twice a day) plus amoxicillin twice a day, and clarithromycin twice a day for seven consecutive days.
Dosage in patients who require prolonged treatment with NSAIDs
If the peptic ulcer appeared from long-term NSAID consumption, 20 mg per day is used for four to eight weeks, depending on the progress of ulcer healing.
Contrariwise, if you want to prevent ulcers while taking NSAIDs, take 20mg a day every day you take NSAIDs.
Dosage in Zollinger-Ellison syndrome
In this particular situation, the suggestion is to make a staged treatment starting with 40 mg twice a day and then adjust it according to the needs of each patient. Other people will likely need up to 160 mg per day.
Can I take Nexium with meals?
Nexium pills should be taken with liquids, better with water. They should not be chewed or crushed, only swallowed.
The idea is that they should be taken on an empty stomach, especially in the mornings when you get up and wait about 20 minutes before to start your meal.
The tablets can be dispersed in non-carbonated water and deposited by gastric tube in patients with swallowing problems. It can only be dissolved in non-carbonated water because the tablet may lose its special coating and have no effect in the body if it is mixed with different beverages.
How long should I take Nexium?
The treatment time will depend on the doctor's prescription and the disease and its severity, according to the schemes described in the dosage section. The standard treatment is not to be prolonged beyond eight weeks.
When does Nexium start working?
Esomeprazole has the benefit that its effects begin within 1 hour of taking it, and these results can last for hours, which is one of the positive features of this drug.
Efficiency and safety: Why choose Nexium?
Many scientific studies support the use of Esomeprazole due to its high efficacy and safety. One of them is the one carried out by the scientists' Sung and Barkun, where they confirm that Esomeprazole significantly reduces the number of bleeding patients with bleeding ulcers and shortens the time of clinical stay of patients needing intravenous treatment.
Another interesting study confirms that the gastric acid control achieved with Esomeprazole is higher, faster, and longer-lasting than with any other proton pump inhibitor, a beneficial result not only for the treatment but also for the patient's savings. The longer the results, the fewer pills are needed to relieve the symptoms.
The cure rate of peptic ulcers is almost 90%, according to European researchers.
Multiple clinical trials have tried to compare the effectiveness of esomeprazole versus lansoprazole, but unfortunately, no difference has been found in either symptom relief or healing rate, so both drugs are equally effective.
Finally, a comparative study between omeprazole and esomeprazole confirmed that the elimination rate of esomeprazole towards H. pylori was higher. This is attributed to the fact that it provides superior gastric acid control for more hours than classic omeprazole, making it more potent and effective, promoting better clinical response and a higher recovery rate.
We cannot finish without mentioning that this medication can not only provide you with a faster and more effective recovery, but it is also generous with your savings. And in the end, the benefits go beyond a good response to the treatment.




Stomach ulcers are a silent but quite common problem
Have you ever felt a burning stomach, heartburn, or chest pain? If the answer is yes, then you are probably suffering from a gastric ulcer. Gastric ulcers, also known as peptic ulcers, are a common but silent problem today. Many people notice the symptoms, while others gently experience only one of them.
The frequency in the world population is between 5 and 15%, but this depends on the diagnosis frequency.
These incidence rates are approximate and are not assimilated to the real values since many people suffer from peptic ulcers but do not go to the doctor.
Gastric ulcers are a condition that is not conditioned by gender, race, or age; most of the medical profession suffers from this disease, taking into account that they are the first to know how to prevent it.
These wounds can change their name depending on where they appear, with the duodenal ulcer being more frequent than the gastric one according to multiple studies over several years.
The life quality of those who suffer from stomach ulcers decreases considerably over time. The person who suffers this condition has to deal daily with stomach discomfort and digestion problems. For them, eating can become a nightmare.
But what are gastric ulcers really?
They may also be named gastroduodenal ulcers according to where they are located. An ulcer is a deep, undermining lesion in the walls of the stomach, significantly compromising its architecture and deep layers.
We must explain the anatomy of the stomach so you can understand it better. The stomach is composed of four layers, the mucous layer being the most superficial and the one that is in contact with all the food and substances that we ingest daily.
It follows the submucosa after the mucosa, then the muscle layer, and the serosa. All these layers have specific functions; the muscular layer, for example, is responsible for making the necessary movements to help digestion.
Gastric ulcers generally affect the mucosal layer because it is the first of all. The rest of the layers can be damaged if the wound does not improve and progress.
The mucous layer is the leading character in this section. In it are found glands of different sizes and functions that work endlessly to produce the gastric juices needed in the digestion.
At the same time, this layer is separated into several sub-layers, similar to the skin. The mucosa is subdivided into the epithelium, connective tissue, and muscle. For now, we will focus on the epithelium since it is necessary to know its function in the body to understand the rest of this article.
Do you remember when you were taught the digestive system in school? Well, neither does us, so let's take a look at it. In the epithelium of the stomach mucosa, there are essential cells for digestion and protection of the stomach; we can mention among them the parietal cells, principal cells, and endocrine cells.
The main job of the parietal cells is to produce hydrochloric acid, while the principal cells make enzymes that promote the breakdown of the food we eat. These enzymes are the ones that attack the food and turn it into a mess inside our stomach.
Endocrine cells also have a key role; they produce hormones (as their name suggests) that function as an appetite alarm when released into the blood. These hormones briefly are what induce appetite and are released according to the daily needs of the body.
| S.No. | Ingredients | F 1 | F 2 | F 3 | F 4 | F 5 | F 6 | F 7 | F 8 |
|---|---|---|---|---|---|---|---|---|---|
| Drug loading stage | Q/mg | Q/mg | Q/mg | Q/mg | Q/mg | Q/mg | Q/mg | Q/mg | |
| 1. | Esomeprazole sodium | 45 | 45 | 45 | 45 | 45 | 45 | 45 | 45 |
| 2. | Mannitol (PerlitolSD 200) | 90 | 45 | 45 | 45 | 45 | 45 | 45 | 45 |
| 3. | Mannitol (PerlitolSD 200) | – | 44 | 44 | 43 | 43 | 48 | 50 | 50 |
| 4. | Kollidon CL | 1.5 | 1.5 | 1.5 | 3.0 | 3.0 | 3.0 | 3.0 | 3.0 |
| 5. | Sodium lauryl sulphate | 1.55 | 1.55 | 1.55 | 1.55 | 1.55 | 1.55 | 1.55 | 1.55 |
| 6. | Povidone (PVPK-30) | 15 | 15 | 15 | 15 | 15 | 10 | 8 | 8 |
| 7. | Sodium carbonate | 10 | 10 | 10 | 10 | 10 | 10 | 10 | 10 |
| 8. | Calcium stearate | 1 | 1.5 | 1.5 | 1.5 | 1.5 | 1.5 | 1.5 | 1.5 |
| Subcoating Stage | |||||||||
| 9. | HPMC (5CPs) | – | 17.5 | 17.5 | 17.5 | 13 | 13 | 13 | 13 |
| 10. | Sicovit yellow | – | 0.8 | 0.8 | 0.8 | 0.6 | 0.6 | 0.6 | 0.6 |
| 11. | Propylene glycol | – | 1.5 | 1.5 | 1.5 | 1.0 | 1.0 | 1.0 | 1.0 |
| 12. | Titanium dioxide | – | 0.4 | 0.4 | 0.4 | 0.3 | 0.3 | 0.3 | 0.3 |
| 13. | Purified water | – | 175 | 175 | 175 | 130 | 130 | 130 | 130 |
| Enteric coating stage | |||||||||
| 14. | Eudragit L30D55 | – | 27.0 | 33.12 | 33.12 | 33.12 | 33.12 | 33.12 | 33.12 |
| 15. | Triethyl citrate | – | 1.0 | 1.73 | 1.73 | 1.73 | 1.73 | 1.73 | 1.73 |
| 16. | Polysorbate 80 | – | 0.3 | 0.5 | 0.5 | 0.5 | 0.5 | 0.5 | 0.5 |
| 17. | Purified water | – | 60 | 60 | 60 | 60 | 60 | 60 | 60 |
| F = Formulation Batches | |||||||||
Why do I need this information? To find out how an ulcer happens
Once we know the anatomy and normal function of the stomach, we can talk about how ulcers occur. The process by which an ulcer is produced is a bit complex, but here we can make it easier.
To start on the right foot, we must understand that there is no single reason for an ulcer to take place; on the opposite, there are many reasons, and the causal mechanism will depend on the main reason.
We will only take into account the most worldwide common causes, which are ulcers due to the consumption of NSAIDs such as ibuprofen, naproxen, ketoprofen, diclofenac sodium, or potassium, aspirin, and acetaminophen, and ulcers caused by the infection of dangerous bacteria called Helicobacter pylori. Both of these mechanisms are quite interesting. Read on to learn about amazing things.
NSAIDs produce damage to the stomach because they interfere with the process of making necessary substances for the protection of the stomach, mainly in the production of mucus. The human body is wise and developed a system that could protect the stomach because it knows it is an acidic and potentially erosive medium.
This protection system is given by the mucous cells of the stomach, remember we mentioned them? They produce mucus that allows protecting the underlying layers of the erosive acid that is released daily in the stomach.
The problem appears when the cells that produce mucus stop producing it, leaving the hydrochloric acid in contact with the walls of the stomach. Drugs such as ibuprofen or acetaminophen inhibit the chemical processes of the cells that produce this mucus because they interfere with the production of prostaglandins.
About 70% of patients who use NSAIDs indiscriminately will have some degree of gastrointestinal damage, but not all patients are aware of this.
There is no non-steroidal anti-inflammatory drug that is free from the risk of digestive complications, which is why it is vital to reduce the consumption of these drugs only when it is strictly necessary.
The other very common cause is a gastric infection by the germ Helicobacter pylori. In this part, we want to insist because this bacterium is intimately related to the occurrence of gastric cancer, so prevention is the key.
This microorganism is in our body in natural situations; we all have H. pylori because it is part of the natural microorganisms that make us up as human beings. The issue is when there is an imbalance of the bacteria and its amounts, or rather when there is an increase in its load.
H. pylori can be in the water we drink or in the food we eat, many foods can have it, and we have contact with it since we are children starting feeding!
After entering the mouth, it travels through the entire upper digestive system until it reaches the stomach, where it adheres to and colonizes its walls. The damage it produces is because it not only attacks the protective elements of the stomach but also inhibits the production of hydrochloric acid to avoid being degraded by it. It is a quite intelligent bacterium!
Hydrochloric acid also works as a protective method against certain bacteria since some of them cannot live in acidic environments. Because H. pylori are more dangerous than it seems, it takes full advantage of its powers and destroys the second protective mechanism of the stomach, the acid.
In this way, the bacteria not only attack the protective machinery but also begin to destroy the cells of the gastric walls, giving rise to a deep ulcer causing the annoying dyspeptic symptoms.
We can fall short of talking about this exciting topic, but the main thing you should understand is that both NSAIDs and H. pylori bacteria are the most common triggers of gastric ulcers in the world.
There are other triggers, including Zollinger-Ellison Syndrome, stress ulcers in hospitalized patients, and some factors that increase the risk for an ulcer to appear, such as excessive alcohol consumption, smoking tobacco, and drinking too much coffee.
What are the symptoms?
The most frequent symptom and the one we should always be aware of is the feeling of discomfort in the upper abdomen, where the stomach is, which improves with the consumption of food and commonly reappears a few hours later.
This annoying feeling can sometimes be disabling and wake you up in the morning. This symptom appears in almost 90% of patients, and all patients describe it as a burning pain.
Other symptoms are nausea and vomiting this as a result of heartburn and pain, also coughing, gas and weight loss. Gastroesophageal reflux is another described symptom, associated with pain in swallowing due to reflux when acid rises in the throat, and heartburn.
What tests are used to confirm an ulcer?
Your doctor will probably order routine laboratory tests to assess your overall condition, including blood tests like hematology.
For a gastroenterologist to make a diagnosis of peptic ulcer, it is required to perform imaging studies of the upper digestive tract, with digestive endoscopy being the main test.
Upper endoscopy is a study that explores the stomach, duodenum, and first part of the intestine; this is thanks to a small device called an endoscope that passes through your mouth to the areas to be studied.
The endoscope is flexible and small and contains a camera that allows the doctor to see the stomach on a large screen, making the job easy for the doctor.
Once the stomach ulcer has been confirmed, you should have a laboratory test and biopsy to look for H. pylori to conclude that it is the primary cause.
How is the treatment?
The treatment can change based on the cause of the ulcer, and it is necessary to comply with all the steps for its success.
You should stop the medications when the ulcer is caused by the indiscriminate taking of NSAIDs, along with daily use of proton pumps inhibitor drugs such as Omeprazole, Lansoprazole, or Esomeprazole.
When the cause is infectious by H. pylori you can take triple therapy with antibiotics and proton pump inhibitors.
This treatment is based on the simultaneous consumption of Omeprazole-derived pump inhibitors plus Clarithromycin and Amoxicillin for seven or fourteen days, depending on what your doctor says.
The cessation of substances such as coffee, alcohol, and tobacco is required since it has been shown that ulcers are 30% more frequent in people who smoke, drink a lot of coffee, or drink alcohol several times a week.
Can I treat an ulcer naturally?
The answer is no. Many natural options can alleviate the symptoms, such as drinking water with bicarbonate; or drinking milk; however, they are not the solution to your problem.
On the contrary, what they do is extend the illness because as long as you feel well, you will not have the urge to consult a doctor.
If you do not go to a doctor, you may suffer serious complications such as bleeding, and ulcer perforation, which occur when the depth of the ulcer hole is such that it reaches the blood vessels. So don't prolong it any longer; go to your trusted doctor and start treatment!
What is the prognosis?
This condition usually has a good prognosis, provided that the proper dietary and therapeutic measures are taken. For this, you should not return to consume the things that give you gastric discomfort; the ulcer will likely reappear if you do.
How long does the treatment last?
This question relies on many things but mainly on the experience of the doctor, his indications, the severity of the ulcer, and finally, the cause.
Sometimes four weeks are necessary for some patients, while others may need eight weeks of treatment; this varies according to each person's improvement.
You probably finish the treatment, and the ulcer persists; this is because the healing is slower than the treatment, so you have to let it flow and be patient.
What should I stop eating to get better?
Well, nothing, the food is free, although if you recognize the foods that make you sick, you should stop them, and as we have already mentioned, you should not consume alcohol or caffeine.
Are there other complications besides the bleeding?
Of course, the more advanced the disease, the more complications there will be. The main consequence is ulcer bleeding. Bleeding can arise in up to 15% of patients, according to studies.
It usually appears in older people over 65 years old. The usual symptoms are brown vomit, blood in the feces, tachycardia, and shock when it is serious.
Perforation is the second complication, and it appears when the ulcer has become so deep that it has broken the stomach wall. The symptoms are severe abdominal pain, bleeding, decreased blood pressure, and shock.
Another rare complication is bowel obstruction. When an obstruction happens it is related to chronic disease probably caused by gastric cancer. Only 2% of patients with ulcers develop pyloric obstruction.